
Redesigning the Postpartum Experience with Minority Women in mind
Tools: Claude, FigmaAI, FigJam
Role: UX Designer
Status: Concept Design 2026
Focus Areas: Healthcare UX, Maternal Health
Timeline: 5 days
Responsibilities: Research, Interviews, UX Design, Rapid Prototyping, and Usability Testing
Personal Context
My daughter almost didn’t get to know me.
In 2025 I gave birth and was sent home with a clean bill of health. Then two days later, I ended up back in the hospital, where I stayed for a week… diagnosed with severe postpartum preeclampsia.
This project started as a personal reckoning and became a research question: what would it look like to design a postpartum experience that does not rely on luck? One that sees minority women — especially Black women — before a crisis occurs rather than after?

Key Research
60% more likely
Black women's risk of developing preeclampsia compared to white women.
24%
of Black women had persistent heart dysfunction at 6–12 months postpartum. Only 2% of white women.
17.1
strokes per 10,000 deliveries for Black women with preeclampsia. 6.5 for white women.
40%
of women nationally never attend a postpartum visit at all.
*All References can be found at the end of this case study

"I kept telling them something felt off before they sent me home. The nurse said it was normal new mom stuff. I didn't want to be dramatic so I didn't push it"
— Aaliyah, 32, first-time mother, Atlanta GA.
Readmitted 5 days postpartum with preeclampsia.
Findings
Based on research and user interviews I conducted, I chose to focus the initial design on the following points:
🧗♀️
Discharge is a cliff, not a transition
Every participant described going home as a sudden removal of support rather than a managed handoff.
⏳
The six-week gap is where the danger lives
The most critical window for postpartum complications — cardiovascular crisis, preeclampsia onset, mental health deterioration — falls almost entirely within the first three weeks. Yet the standard follow-up appointment is scheduled at six weeks
✨
These women knew their bodies.
Across all three interviews, participants described suppressing their own knowledge in medical settings — not pushing back, not wanting to seem dramatic, not having the language to be taken seriously.
Solution
An application that meets new mothers at the most vulnerable moment of their postpartum journey. Replacing the generic hospital discharge packet with a personalized, AI-assisted experience that speaks plainly, monitors intelligently, and connects her to human care before something becomes a crisis.
Warm
Proactive
Personal

Text here
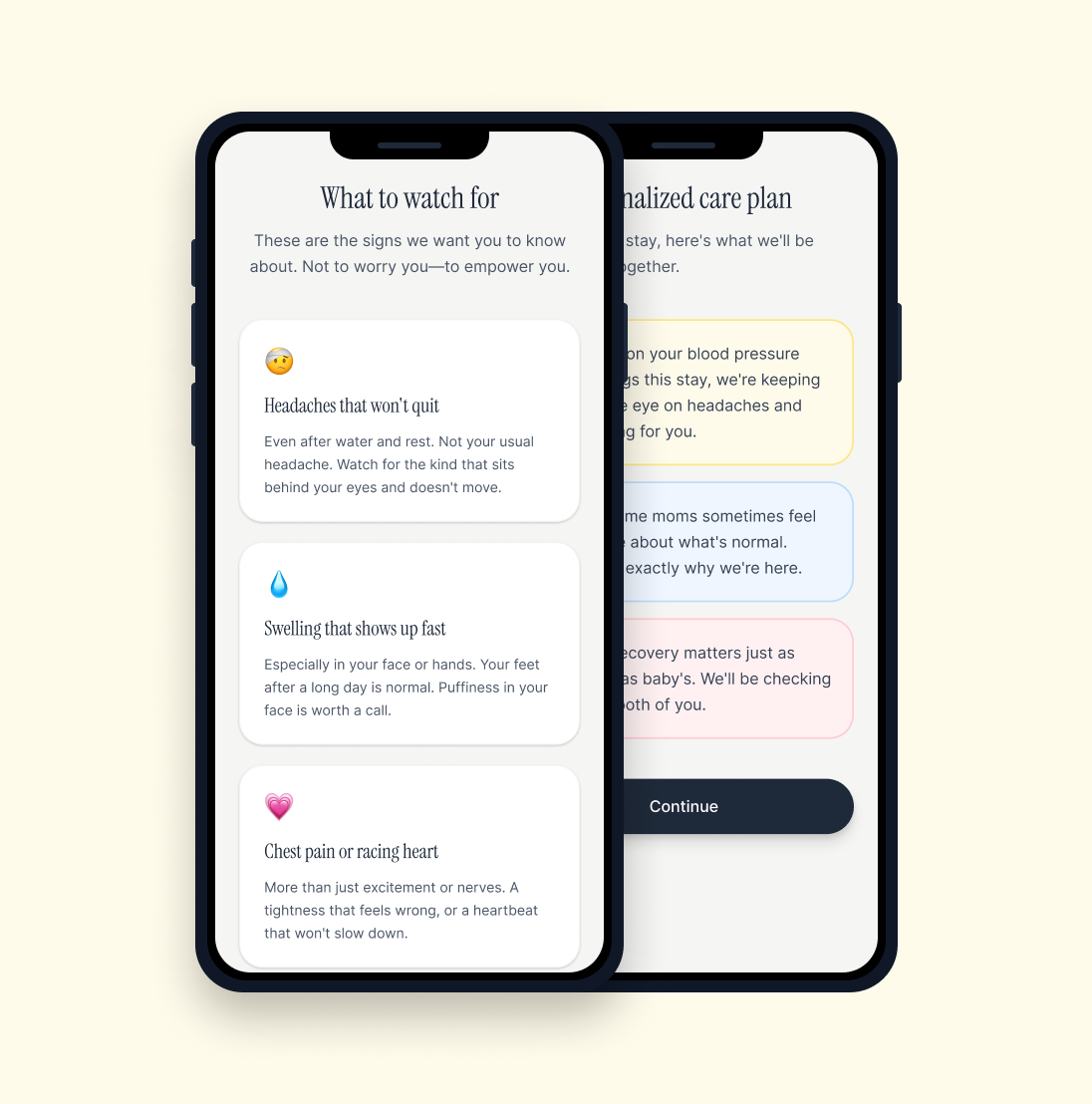
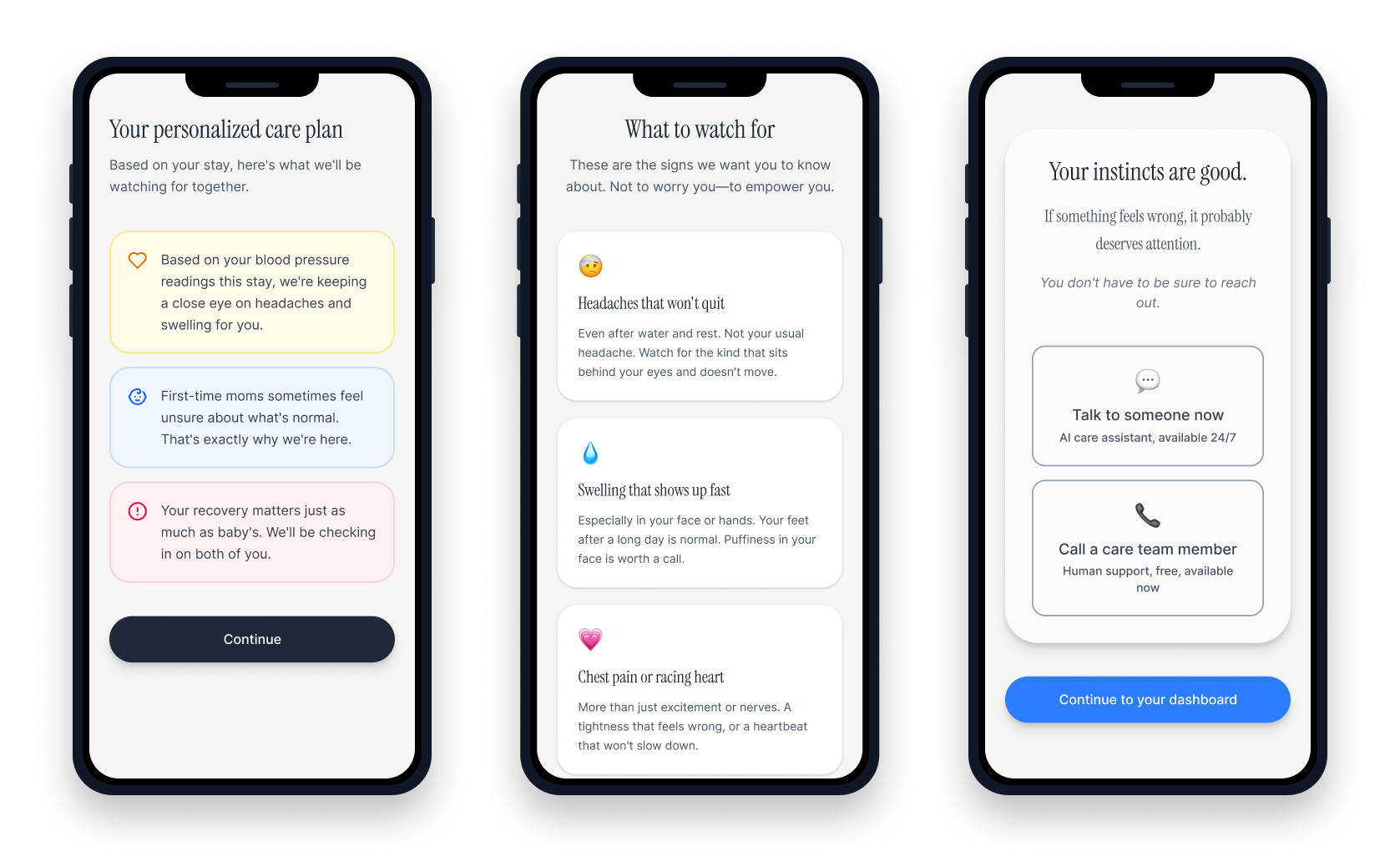
Discharge Flow
Displays personalized risk indicators drawn from the patient's health history and hospital stay, so she leaves with context specific to her, not a generic checklist
Translates clinical warning signs into plain, human language that feels like a trusted friend explaining what to watch for, not a pamphlet
Closes with an emotional anchor that validates her instincts and gives her two equal-weight paths to support, AI or human, with no friction between them
Transitions her directly into a dashboard built around ongoing care, not a one-time handoff
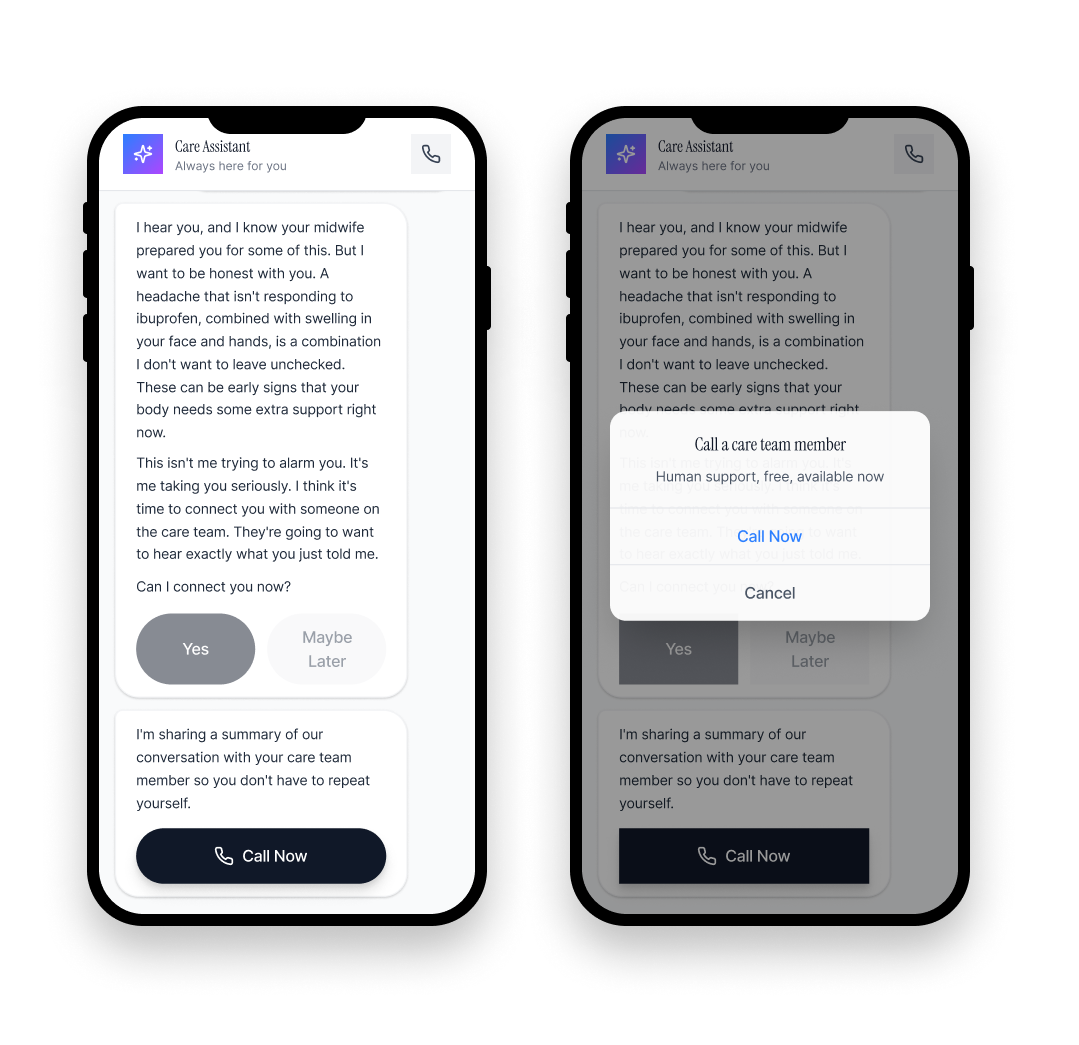
Check In Flow
Opens with a time-based, personalized prompt that signals the system has been paying attention since she got home
Follows her responses adaptively, staying with what she just shared before moving to the next question
Names uncertainty honestly and communicates concern without alarm, honoring what her care team told her while flagging combinations that warrant attention
Escalates to a human care team member at the right moment, and shares a conversation summary so she never has to repeat herself
💭 Reflection
What This Taught Me
This case study began with a personal experience and became something larger. Researching the data behind what happened to me, and to many others, was not comfortable. The missed diagnoses, the miscalibrated tools, the documented bias. But it was clarifying.
The most important thing I learned as a designer is that the solution was never going to be a beautiful interface.
It was going to be the right information reaching the right woman at the right moment, in a form she could actually use. Sometimes that’s a message. Sometimes it is a person who speaks her language. Sometimes it is simply being believed.
Next steps:
This prototype was intentionally created using AI tools to rapidly turn the concept into a testable prototype. Next, I would stress test the design by putting it in front of real women who recently gave birth and have them provide feedback.
If this was for a specific brand, I would also document the design patterns and AI interaction principles that emerged from this work into a reusable framework for future projects.
References & Further Reading
The following sources informed the data presented in this case study.
Preeclampsia & Maternal Mortality
1. Healthcare Cost and Utilization Project (HCUP) — Black women 60% more likely to develop preeclampsia.
Agency for Healthcare Research and Quality, 2017. pmc.ncbi.nlm.nih.gov/articles/PMC4782921/
2. A Critical Review on the Use of Race in Understanding Racial Disparities in Preeclampsia — 41.4% misclassification of Black women using standard proteinuria screening.
PMC/NCBI. pmc.ncbi.nlm.nih.gov/articles/PMC8516080/
3. U.S.-Born Black Women at Higher Risk of Preeclampsia — Black women 3–4x more likely to die from pregnancy-related causes.
Johns Hopkins Medicine / JAMA, December 2021. hopkinsmedicine.org/news/newsroom/news-releases/2021/12/us-born-black-women-at-higher-risk-of-preeclampsia-than-foreign-born-counterparts-race-alone-does-not-explain-disparity
4. Does race or ethnicity play a role in the origin, pathophysiology, and outcomes of preeclampsia? — Hospital readmission rates 6.8 vs 1.7 per 1,000; postpartum follow-up rates 47% vs 70.5%.
American Journal of Obstetrics & Gynecology, 2020. ajog.org/article/S0002-9378(20)30769-9/fulltext
Peripartum Cardiomyopathy
5. Racial disparities in peripartum cardiomyopathy: eighteen years of observations — 24% of Black women had persistent heart dysfunction at 6–12 months vs 2% of white women.
PubMed, 2020. pubmed.ncbi.nlm.nih.gov/32508175/
6. Disparities in Cardiovascular Disease Outcomes Among Pregnant and Post-Partum Women — Black women 1.71x higher odds of peripartum cardiomyopathy.
Journal of the American Heart Association, 2021. ahajournals.org/doi/10.1161/JAHA.120.017832
7. Comparison of Clinical Characteristics and Outcomes of Peripartum Cardiomyopathy Between African American and Non-African American Women — Black women diagnosed later, presented with more severe disease, recovered less frequently.
JAMA Cardiology, 2017. jamanetwork.com/journals/jamacardiology/fullarticle/2657313
Stroke
8. Hypertensive disorders of pregnancy and risk of stroke in U.S. Black women — 66% increased long-term stroke risk in Black women with hypertensive disorders of pregnancy.
PMC, Black Women's Health Study. pmc.ncbi.nlm.nih.gov/articles/PMC10919377/
9. ACOG Committee Opinion No. 736: Optimizing Postpartum Care — more than half of postpartum strokes occur within 10 days of discharge.
American College of Obstetricians and Gynecologists, 2018. acog.org/Clinical-Guidance-and-Publications/Committee-Opinions/Committee-on-Obstetric-Practice/Optimizing-Postpartum-Care
The Follow-Up Gap
10. ACOG Redesigns Postpartum Care — 40% of women never attend a postpartum visit.
ACOG News Release, 2018. acog.org/news/news-releases/2018/04/acog-redesigns-postpartum-care
11. ACOG Committee Opinion No. 736 — recommends postpartum contact within 3 weeks, not 6.
PubMed. pubmed.ncbi.nlm.nih.gov/29683911/
Heart Safe Motherhood — Penn Medicine
12. Heart Safe Motherhood Program — 92% text-based monitoring compliance vs 44% in-person; racial disparity in postpartum monitoring eliminated.
Penn Medicine / University of Pennsylvania Health System. pennmedicine.org — search Heart Safe Motherhood